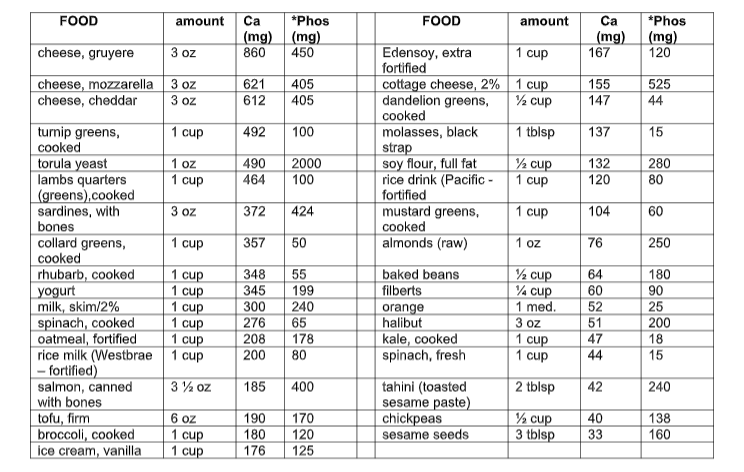
Calcium absorption is regulated by a number of factors; its absorption can be impeded by substances such as oxalates and phytates. Oxalates are found in dark green leafy vegetables – especially spinach, as well as rhubarb where the concentration is relatively high. Phytates are found in whole grains, seeds, nuts and legumes; however, if these foods are sprouted, soaked, leavened (think: sourdough bread), or gently heated phytase (an enzyme naturally occurring in these foods) breaks down the phytates and prevents their interaction with calcium absorption.
Uric acid is a waste product normally present in the blood as a result of the breakdown of purines. Excessive amounts of uric acid can cause crystals to form in the joints, leading to gout. Therefore, a low purine diet will lengthen the time between flare-ups and reduce their severity.
Foods to be eliminated: most fish and seafood, all organ meats and gravy. The following foods are moderately high in purines are to be mostly eliminated. These may be eaten once a month at most:
• anchovies • lamb • veal • bacon • liver • salmon • turkey • haddock * (once a week due to high omega fat content and local fish )
Some vegetarian foods have been linked to higher purine content and are to be avoided on a daily basis including oatmeal, mushrooms, spinach, beans and lentils. These may be eaten maximum once a week.
Foods to include in your diet that are known to counteract the production of uric acid include: cherries, apples, strawberries, blueberries, kale, celery, squash, watercress and avocado.
You will need to increase vegetarian sources of protein – nuts, seeds, avocado, quinoa, and eggs. I recommend 1 cup of whole grains daily (see alternative Grains handout,) a variety of vegetables, fresh fruits, and moderate amounts of dairy products including those sourced from sheep and goat . Also, protein shakes with 2 tbsp of flax oil, fresh/frozen fruit and almond or rice milk or water are beneficial. I like the RAW Protien brand shakes, although plain whey is acceptable. Go to your local health food or whole foods store, buy a number of single serving shakes, and find one you like. Protein shakes are best for post-exercise consumption for muscle gain, or as an easy breakfast.
Once a daily balance of non-purine foods has been incorporated into your lifestyle, begin working on alkalinizing your body’s pH to achieve the optimal acid-alkaline state of health.
Black cherry juice concentrate is well known to counteract gout. Drink 1 cup daily. 8 glasses of water are also required or 1.5 Liters. Also beneficial are nettle or red clover tea, and clover sprouts. Increase turmeric in cooking.
I am giving a webinar this week to a group of cardiologists on all gender cardiology. Spoiler alert, there is no difference between cis and trans gender heart health. The differences lay in access to health care, stereotypes about hormone therapy, and minority stress. For cardiology, once you have a sick heart, regular physician follow up is crucial to your care – multiple medications are sometimes needed to improve or preserve heart function and imaging is needed over a lifetime to track structure and function. If a person does not feel safe at their cardiologist’s office because they are constantly called the wrong name or experience microaggressions about their body, that person will avoid going back or drop out of care all together. Therefore, the first and most important point of all gender cardiology is creating a safe medical home with dedicated staff and physician training in transgender and gender diverse specific health care.
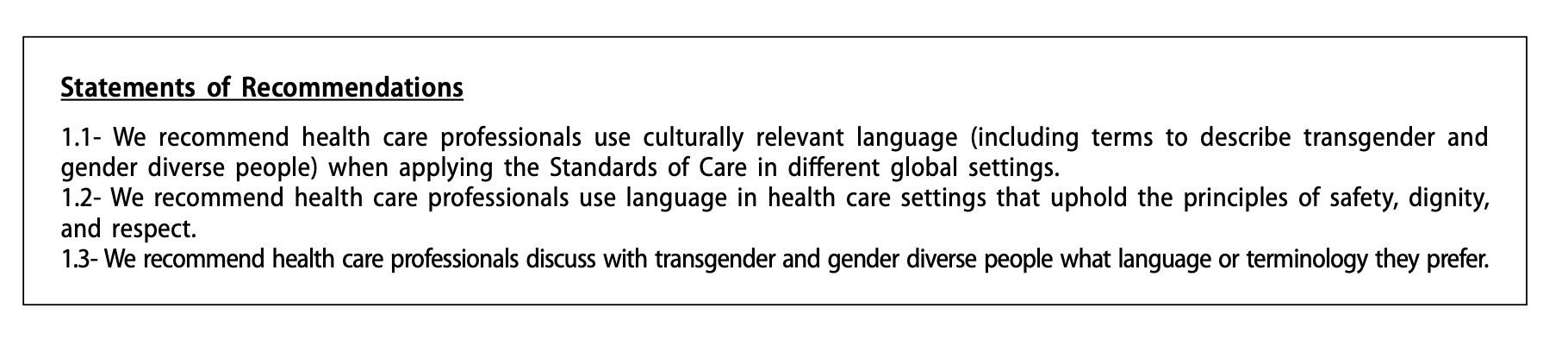
Documentation matters. Medical charts are living documents of a patients experience and how we represent someone matters both for the patient and for all the people who read the document. Safety, Dignity and Respect are basic human rights which are not always upheld for gender diverse individuals, even in a doctors office. Do not be afraid to ask an individual what terms, names, pronouns they would like used in their chart. Asking is consent and consent is powerful. Some terms have fallen out of favor over the last 2 decades that I frequently hear used in the hospital such as Male-to-Female (MTF) and Female-to-Male (FTM). These have been replaced with assigned gender at birth attached to current gender presentation, or just gender presentation. Assigned gender at birth includes Assigned Female at Birth (AFAB) and Assigned Male at Birth (AMAB.) These can be helpful in a medical setting bc they may signify reproductive organs present ( or they may not depending on surgical interventions.) Some gender diverse folks feel passionately against AMAB/AFAB as well because they focus more on the assigned birth gender than the current gender. Therefore, in documentation, either ask the patient how they would like to be represented, or consider using a hybrid like AMAB transwoman, or just transwoman in your notes.
Cardiology and IM are frequently consulted for assessment prior to surgery. Treat gender diverse folks the same as you would anyone else. For a long time gender affirming hormones were stopped prior to surgery, especially estrogen for transfeminine patients due to the heightened risk of venous thromboembolism. This practice is no longer recommended. We would not put a cisgender person on hormone blocking agents for a surgery; therefore, stopping all hormone treatment for transgender individuals does not make sense. In fact, continuation of hormone treatment is beneficial for withdrawal prevention, mental health and for prevention of side effects of hypogonadism including osteoporosis. Continue the current therapy through surgery and risk stratify/ treat perioperatively as you would any other patient with RCRI, MINS screening and DVT prophylaxis.
“Hontscharuk and Schecter assemble the most comprehensive review of literature from plastic sur- gery, gynecology, and endocrinology to consider the risk profile of transgender hormones and surgical venous thromboembolism. One surprise of their well-sourced study is that the risk of perioperative estradiol may be lower than commonly thought. High rates in early series are attributed to the use of oral ethinyl estradiol and high doses, with newer regimens showing lower rates. One area where the literature is limited, however, is in quantifying cur- rent practices in hormone cessation. In a survey of six high-volume vaginaplasty centers (unpublished data), all surgeons still stopped estradiol 2 to 4 weeks before surgery.”
Ok, now we can finally start talking about the heart and gender affirming hormones, starting with testosterone. This topic applies to anyone who has testosterone including cisgender men but is specifically for transmen and nonbinary people using testosterone. As the rise of ‘andropause” or mens antiaging medicine came into the public eye, the medical assumption was that because men had more cardiovascular disease (CVD) and men had testosterone, therefore testosterone increased heart disease risk. This was pure conjecture and has not held up in any evidence based investigations. A 2014 JAMA article was published from VA data-mining that stated that hypogonadal men starting testosterone had increased risk of MI, with the declaration that therefore testosterone was not indicated in anyone with increased cardiac risk or cardiac disease. The article was quickly retracted and amended as the data was corrupted (multiple patients with MI’s had not started the testosterone, ciswomen not on testosterone were included in the MI population.) The damage was done, and many people still believe the false claims a decade later.
Testosterone therapy is vital for gender diverse patients who need masculinization. Even if it did carry a CVD risk, the beneficial effect of mental and physical wellness for gender congruence would be worth the possible risk. Because of its importance in transgender medicine, this is an ongoing hot topic of research to better understand the nuances and possible risks of testosterone therapy.
“A large 2018 case control study from several US centers that used 10:1 cisgender matched controls found no statistically significant difference in rates of MI or stroke between transgender women and cisgender men, a rates of MI, stroke, or venous thromboembolism (VTE) between transgender men and cisgender men or women. There was a statistically significant hazard ratio of 1.9 for VTE among transgender women when compared with cisgender men.” CH 15 WPATH SOC
The relationship between testosterone and trans health is important enough that the American Heart Association investigated and released a scientific statement in 2021, because trans and gender diverse folks of all genders HAVE consistently had worse cardiovascular morbidity and mortality than age matched peers.
The bottom line ” Mounting research has revealed that cardiovascular risk factors at the individual level likely do not fully account for increased risk in cardiovascular health disparities among people who are TGD. Excess cardiovascular morbidity and mortality is hypothesized to be driven in part by psychosocial stressors across the lifespan at multiple levels, including structural violence (eg, discrimination, affordable housing, access to health care). ”
However, in the anti-aging and cisgender mens health community the question of cardiac safety with testosterone hormone replacement lingered. In 2015 after the original data debacle, the FDA required companies making approved testosterone products to participate in clinical trials to elucidate the evidence. The Testosterone Replacement Therapy for Assessment of Longterm Vascular Events and Efficacy Response in Hypogonadal Men (TRAVERSE) trial was created and just published in 2023.
Bottom line? Testosterone repletion to biological levels for cisgender men did not increase cardiovascular risk, with primary endpoints of the study being first occurrence of any component of a composite of death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke. A secondary cardiovascular end point was the first occurrence of any component of the composite of death from cardiovascular causes, nonfatal myocardial infarction, nonfatal stroke, or coronary revascularization, assessed in a time-to-event analysis.
Testosterone HAS been repeatedly shown to decrease HDL, the protective scavenging cholesterol and increase triglycerides. It evidences variable effects on total cholesterol and LDL . This could be a piece of the puzzle for increased CVD risk in trans men, but has not been definitively proven yet. Regardless, exercise is the best way to increase HDL in all genders, so as health care providers we need to continue motivational interviewing for active lifestyles, 150minutes of exercise weekly and lipid-conscious nutrition for all our patients including trans men.
So why are transmen more likely to have cardiovascular disease? The the answer is multifactoral and boils down to lifestyle and and health care access which crosses many intersections of class, and race, minority stress and more (which is another important conversation). Heart disease is a cumulative pathology. Unless one has a congenital heart condition, it takes decades of uncontrolled alcohol use, dysregulated blood sugar, nicotine toxicity, low nutrient and high fat foods and sedentary lifestyle to generate atherosclerotic coronary disease. Prevention is the best medicine for a healthy heart and vasculature, but prevention also means having a doctor to work with for things like blood work and blood pressure measurement. If you are someone who has a bad experience in the medical world, or worse, someone who is denied care due to your gender or sexuality, that person will often have worse outcomes with age.
TBC in the next post – ESTRADIOL! – because this one is getting long!
I had the good fortune to be profiled in Society for Hospital Medicine’s LGBT postings this June 2023 as part of Pride Month. I was interviewed early in the Spring and received a preview of the article. The journalist stated that I did pronoun advocacy work and received the Diversity and Equity Award for my Residency class for pronoun work in the EMR. This is not true. The language from the first draft shifted just enough in the final version to have a different meaning. When I saw it in print I became VERY uncomfortable with the inaccuracy. I did not remember that point in the draft. I went back to the email exchange and indeed it was there from the beginning. It is strangely ironic that I would be highlighted as the pronoun advocate in medicine because of the very real pain that I have caused other people by mis-pronouning and misgendering them.
Although I have been involved in trans health advocacy since 2003 I have made many mistakes over the past two decades. In 2013 I gave a talk at the Philadelphia Health Conference that was disastrous; I horribly publicly misgendered several people when calling on them for questions. In 2021 I dated someone that had several GenZ friends who used they/them pronouns and we all struggled with my default to binary pronouns in unthinking moments. Therefore, to have me championed as a pronoun advocate is more bitter than sweet.
I do prefer the gender affirming pronouns of they/themme for myself. I only allowed myself to come into these pronouns in 2021 after over a year (decade) of introspection and examination. The above GenZ folks as well as social media sites like @seedingsovereignty on Instagram helped me realize that even though I have lived most of my GenX life without language to describe my gender I am free to use whatever pronouns that feel most comfortable. I have them in my work signature but I have not pushed for them personally.
The Trans health work that I do includes peer to peer level discussions about language in documentation as many health care providers still use language from the 1990s. I provide trauma informed care for my patients of all genders, and have a special place in my heart for all gender nonconforming folks in health care settings. I work with administrative staff, creating education about the gender spectrum and experience of gender and sexual diverse individuals to create safe medical homes for LGBTTIQ2S folks. And, moving forward I am working to create Justice/Equity/Diversity/Inclusion community gatherings within internal Medicine to lift the voices of Black, Indigenous and Trans physicians towards leadership roles as these are the least represented identities in medicine (and therefore the most needed.)
Some people fall asleep fine but cannot stay asleep. Like other sleep pathology this can be due to a complex interplay of underlying reasons. Often the 24H cortisol circadium rhythm has become dysregulated and the early morning peak is coming earlier than it should, waking people up at 3, 4 or 5am. What can be done? There are some prescription sleep medications that can be helpful, and global stress management skill building is also important. Underlying anxiety disorder may need to be treated and substance use disorders are also major players in sleep-wake disorders.
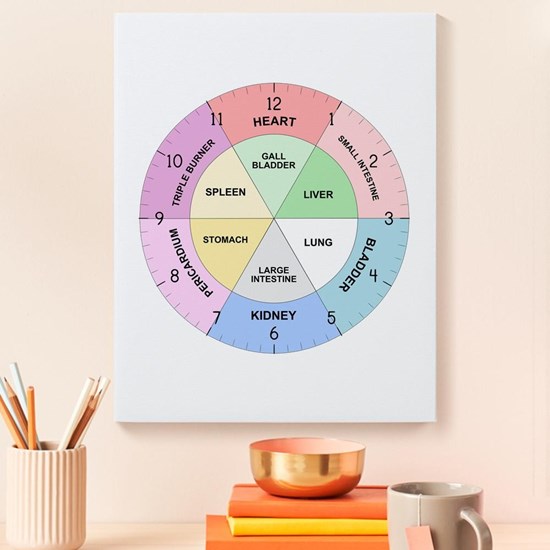
Alcohol is an obvious player in the 3am waking game. For people who drink regularly, depending on what time one goes to bed and therefore stops drinking, at some point the alcohol with start to wear off and the withdrawal will start bringing agitation, heart palpitations, sweating, and headache. This can cause early morning waking between 3-5am. Chinese medicine correlates each organ to a 24H clock, and this time of day is the Liver time. Ironic, yes? Accurate, yes? Decreasing evening alcohol can certainly result in better sleep. Alcohol free evenings may take some time to produce better sleep but after about 7 days of abstinence the sleep cycle will begin to regulate. If full abstinence is not desired, start by at least assessing the effect of alcohol and considering your own motivations for changing drinking patterns as they do certainly effect sleep negatively. Having some protein closer to bed time can be stabilizing to blood sugar and alcohol metabolism overnight.
This is true for diabetics as well as for people using alcohol. This is not my area of expertise, but diabetes is related to increased cortisol levels due to the connection between fasting blood glucose, blood sugar, and the liver and pancreas control of blood sugar during the overnight fasting period. There are several studies on sleep disorders in people with diabetes which have evidenced that there are clinical correlations. If you have diabetes and poor sleep, I recommend working with your PCP or Diabetes specialist to make sure your blood sugar issues are not the root cause before moving into more behavioral or psychiatric sleep medications and sleep medicine studies.
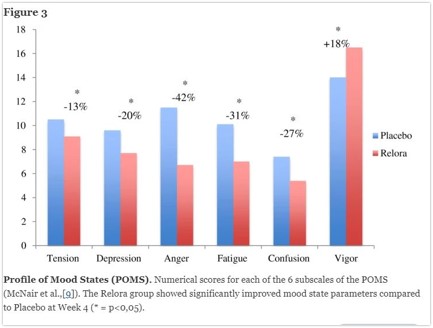
The first botanical medicine I turn to when faced with early waking is a version of several different formulations using standardized botanical extracts of magnolia. The first agent that was trademarked was called Relora and was a Canadian product. This standardized extract regulates disorderde circadiuan rhythms. Whan taken at night it helps smooth out early morning cortisol spikes, decreasing early morning waking related to stress and anxiety. It also has some evidence to decrease stress related eating, and improve subjective mood and wellbeing.
Relora vs placebo effects
A similar American product is Cortisol Manager by Integrative Therapeutics. This product also uses the honokiol standardized extract with magnalol rather than berberine. This product is combined with ashwaganda (Withania somniferol). Ashwaganda also has evidence that it adjusts dysregulated cortisol circadian rhythms for improved early morning waking. There are many sleep formulations available that contain Ashwaganda. Gaia brand “Sleep Thru” formulation is another similar product for use when early waking is the issue rather than difficulty falling asleep.
These botanical formulas are generally safe for people without significant health conditions. If you are taking more than 5 medications, have kidney disease CKL3 or greater, or are on immunosuppressive drugs for transplants, autoimmune disease or any other indication, supplements should not be taken randomly without supervision by a licensed Naturopathic doctor or trained herbalist as there could be real drug-herb interactions.
Finally, as mentioned at the beginning, emotional stimuli do go thru hypothalamic-pituitary-adrenal axis to effect cortisol secretion. Lifestyle modifications are necessary in every case to at least consider the underlying causes of the stress. A pill alone cannot regulate a deeply engrained habit or pattern. Most health care providers would like to hear about what is keeping you up at night, in order to troubleshoot with you ways to improve coping and reduce suffering. These plant based medicines are allies in your journey towards improved health and are only part of the team based approach that real change towards health entails.
lDeshpande A, Irani N, Balkrishnan R, Benny IR. A randomized, double-blind, placebo-controlled study to evaluate the effects of ashwagandha (Withania somnifera) extract on sleep quality in healthy adults. Sleep Med. August 2020;72:28-36.
Talbott, S.M., Talbott, J.A. & Pugh, M. Effect of Magnolia officinalis and Phellodendron amurense (Relora®) on cortisol and psychological mood state in moderately stressed subjects. J Int Soc Sports Nutr10, 37 (2013). https://doi.org/10.1186/1550-2783-10-37
I love falling asleep quickly and easily and waking up 9 hours later.
When this doesnt happen, the work of unpacking the complex architecture of sleep and our associated subconscious and unconscious patterning begins. This post will provide a brief overview of sleep-wake cycle circadian dysregulation as well as nutraceuticals and botanical medicines to help fall asleep. Botanicals to stay asleep or address eearly waking will be in the following sleep post. I will not discuss prescription medications for sleep. Some people with trauma, PTSD, significant depression and anxiety, and persistent insomnia and/or sleep apnea may need pharmaceutical medications for sleep and/or sleep studies to better understand what is happening. Psychiatry, therapy and counselling can also be helpful to do a deep dive into childhood and adult patterning related to sleep or preventing sleep including hypervigilance as well as cognitive behavioral therapy to work with thought patterns preventing sleep.
Everyone agrees that sleep is worse in periods of stress, and sometimes in periods of excitement too. Disturbed sleep is also part of major depressive order for many people with either inability to sleep or desire to sleep too much. And, anyone with a significant grief experience knows that early mornings can be very tough times for waking up and experiencing sorrow. For these reasons and more, treating insomnia is far from simple as sleep is deeply entwined with the conscious and subconscious mind.
There have been many studies on sleep and health outcomes. This 2020 study by Hackett et al states: “Poor sleep quality has been linked with negative health outcomes. Adults who report sleep problems are more likely to have hypertension, obesity and coronary heart disease (CHD) than their counterparts without sleep problems (Koyanagi et al., 2014). Meta-analytic evidence has detected a relationship between short sleep duration and incident hypertension (Itani et al., 2017). However, studies investigating the prospective link between poor sleep quality and hypertension have produced mixed results (St-Onge et al., 2016). Pooled evidence indicates that short sleep duration is a risk factor for obesity (Itani et al., 2017). While poor sleep quality has been linked with the development of the metabolic syndrome in middle-aged and older adults (Troxel et al., 2010).”
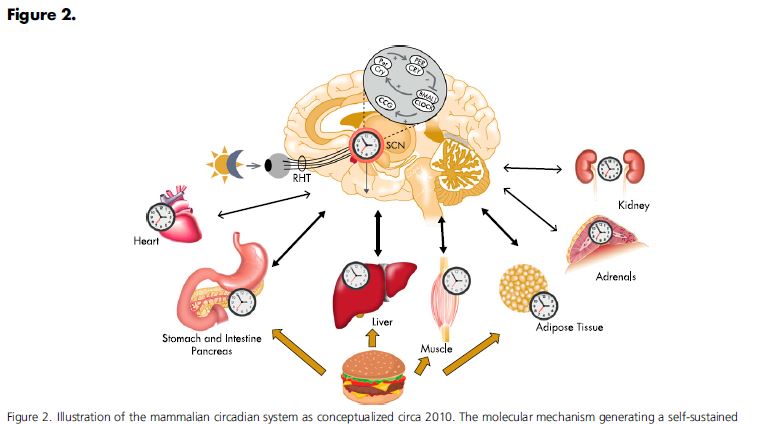
Our bodies hormonal clock may originate in the suprachiasmatic nucleus, but many organs have their own biological rhythms that are regulated independently. This concept has been proven in modern science but orginated in Chinese Medicine more than 5ooo years ago
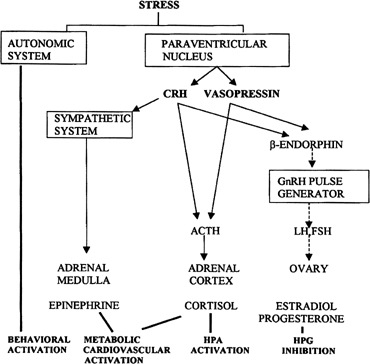
There is a reason we go to sleep at night and wake up in the morning. This is called the circadian rhythm and provides a skeletal structure for many of our hormonal biorhythms. Cortisol and ACTH levels are pulsing throughout the day and night, roughly every 60 minutes. The pulse is generated from within the HPA axis in a dynamic feedback loop. There is a threshold for a negative setpoint that is predetermined by the suprachiasmatic nucleus where ACTH pulses, stimulates cortisol production into the vasculature, which diffuses into the IC space of the brain and stops ACTH production which then retriggers the negative threshold and restarts this ULTRADEIAN cycle. At night (or during sleep hours) the circadean set point is set at a lower free cortisol level in a diurnal pattern.
Living with chronic stress can alter this rhythm. Living with depression can alter this rhythm. Substance use can alter this rhythm. Grief can alter this rhythm. PTSD can alter this rhythm. Changing time zones can alter this rhythm. Shift work can alter this rhythm. Parenting will alter this rhythm. And kids need to develop this rhythm as part of learned sleep patterns coming out of infancy.
So, once ones sleep is dysregulated, what can be done? So-called sleep hygeine is the first step. This is a basic series of actions designed to minimize sleep interruption and maximize comfort and melatonin production. I often tell patients to treat themselves like a 5 years old with a bedtime routine. This creates patterning in the mind and body (those ultradeian clocks) that signals sleep time is coming.
Insomnia falls into to big categories – falling asleep and staying asleep. We will discuss these seperately as they require different medicine.
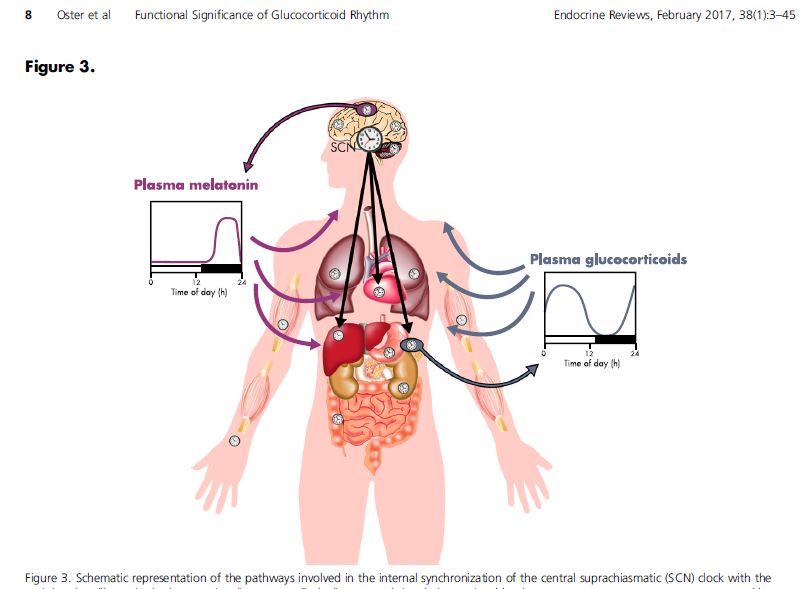
Falling asleep. What a gift it is to drift into effortless sleep. How many times have i lain awake, unable to relax enough to let that sleep veil drift across my consciousness? Falling asleep medicine is often in the form of sedatives in an acute setting. Melatonin + a sedative botanical is a good combination for short or long term difficulty falling asleep. As you can see from the image below, melatonin production has an inverse relationship to plasma levels of cortisol. If your circadian rhythm is dysregulated, melatonin supplementation can help recreate a new pattern (which is why it is used in changing time zones.) In our “more is more” culture people sometimes think taking higher doses of melatonin will work better. In actuality, this pineal gland hormone is naturally microdosed and 1mg is often the best dose. Combining melatonin with an app to provide guided relaxation meditations or sleep-inducing music like binaural beats can increase theta waves at the level of the brain simulating deep relaxation and promoting sleep. (I use the Insight Timer free app almost every night!)
The amino acid tryptophan is converted into 5HTP which is concerted into serotonin which is converted into melatonin. This is the biochemical reason why serotonin deficiency (depression) can lead to insomnia. Increasing foods rich in tryptophan, or taking either SSRI medications or 5HTP supplement can also increase endogenous melatonin production. Do not take 5HTP and prescription mood medications unless prescribed and followed by a health care provider.
My favorite sedative botanicals are valerian (valeriana officionale) and california poppy (Eschscholzia californica). Both are decidedly yucky tasting, with california poppy being super disgusting! However, it is one of the few things that consistently works for me so I choke down the earthy swampy tincture with a juice chaser.
The European union has a formal scientific herbal monograph compendium listing the scientific and traditional uses of 167+ commonly used botanicals. This was originally created to standardize information about commonly used herbal medicines for providers and consumers in an upgradeable format as new evidence develops. I personally prefer the Alt Med review for botanical monographs which is North American but not government regulated like the European compendium. In general herbal medications come in dry form used as teas, preserved in alcohol called tinctures or preserved in glycerine for children or people who cannot tolerate alcohol, capsules of prepared herbs or standardized extract capsules with prespecified amounts of active ingredients in each capsule. The strength of the medicine increases from raw herb/ tea –> glycerite –> tincture –> capsule –> standardized extract as the most potent form.
Valerian is a natural sedative. The active phytochemicals are bicyclic monterpenes, free amino acids, and valepotriates. Valerian is very safe and can be used in pediatrics and pregnancy. I do not reccomend it in late stage kidney disease. If anyone is taking multiple medications with severe illness, please only use any herbal medication under the advice of a naturopathic doctor, experienced herbalist or physician. This plant has stinky volatile oils that are also part of why it works. The herbal chemicals are sedating and calming, they can help both to initiate sleep and to maintain sleep. Start with the lowest possible doses as a tea or low dose tincture (10-30 drops) and increase as needed up to 3 capsules before bed. The primary side effect of valerian is morning grogginess from oversedation. This can be avoided by using lower doses and less potent forms. The smell of valerian could be a factor in ones decision of which to use with glycerite and tincture the least pungent forms.
Valerian (Valeriana officinalis) illustration. Digitally enhanced from our own book, Medical Botany (1836) by John Stephenson and James Morss Churchill.
California poppy is the other sedative plant that I frequently use for my own sleep. I use it in combination with melatonin for shift work and during times of significant stress where I really need something to “knock me out.” It tastes so terrible, but some days that is a small price to pay. I have only found this plant in tincture form. It can be added to a small amount of warm water to evaporate off the alcohol. This medicinal plant is listed in the European compendium as safe for use for adults only with over 30 years of safety. It is not to be used in pregnancy or breastfeeding or for pediatrics as it is in the poppy plant family. It does not have narcotic effects but it does have many chemical alkaloids to induce sedation. It is recommended to be used for up to 2 weeks and then stopping use for at least 2 weeks.
references
Oster H, Challet E, Ott V, Arvat E, de Kloet ER, Dijk DJ, Lightman S, Vgontzas A, Van Cauter E. The Functional and Clinical Significance of the 24-Hour Rhythm of Circulating Glucocorticoids. Endocr Rev. 2017 Feb 1;38(1):3-45. doi: 10.1210/er.2015-1080. PMID: 27749086; PMCID: PMC5563520.
Ruth A. Hackett, Zeynep Dal, Andrew Steptoe. The relationship between sleep problems and cortisol in people with type 2 diabetes, Psychoneuroendocrinology. Volume 117,2020,104688, ISSN 0306-4530, https://doi.org/10.1016/j.psyneuen.2020.104688.
Coming out, even to myself ,as a nonbinary femme has been harder than I expected. I keep waiting for someone to tell me I somehow dont “qualify.” Hell, I question my self on a regular basis, why would I expect less from anyone else?
Many years ago, in the late 90s in Toronto my soon to be best friend Aimée and I would meet for “femme coffee” once a week and talk about the politics, nuances, and intersections of femme identity. I was somewhere between 21-25 and this was all new to me. Pieces fell into place in my psyche connecting me to the this queer community. I was becoming a part of.
Fast forward at least 20 years. Words like genderqueer, nonbinary and ace have flourished in an ever expanding garden of sexual and gender personal affiliations. They/them pronouns are discussed on NPR and the spectrum of trans identity is in media, politics, elementary school and everywhere else. I am in medical school at 45 years old, advancing my personal and professional education in sex and gender health. I am married to an androgynous millennial and she says one night “Femme is not a gender. You have no gender identity.” I was so hurt and angry and erased. I fumbled through my 90s gender books trying to find some proof that I existed; i had no name for who I was.
I folded in on myself at that moment. I knew that I had a complex gender and I knew I existed but I didnt have the words to speak up with.
Current time, or 2020. I was in relationship with another millennial, spending time with their all-trans friend group many of who were GenZ. I am jealous that these humans were able to grow up in a less gendered era than I was and had the freedom to know at 15, or 19, that their internal understanding of their personal gender *as well as their visible identity* could be whatever they wanted it to be. I know in my heart that if I were 17, or 27 instead of 47 I would certainly identify as nonbinary. And maybe I would have pushed my visible boundaries further than I will now.
One friend in particular was classically femme-presenting and identified as nonbinary trans. I repeatedly used she pronouns , probably 50% of the time, as their image in my mind was so deeply ingrained as one pronoun. It felt terrible every time – for everyone involved. I changed to using they/them pronouns for everyone for about 6 weeks until I got used to it as a habit in my mouth and brain. Uncoupling the phenotypical appearance of face/hair/clothing presentation from associated pronouns was very hard work for me. I could not figure out why I was struggling so much: How could i not get this right? What Was Wrong With Me. (spoiler alert: I was struggling with my own gender identity and associated femme biases.)
I wish this friend group and I had been able to have safe gender discussions. I wanted to learn from their growing up experiences as they were obviously very different than mine. I was in a deep struggle with myself as an older AFAB person allowing myself to invoke a nonbinary truth while still presenting as the lesbian femme I have always been. Eventually the words slid into place: I finally had language for a gender that fit my folded up erased insides. I harmed this friend by not seeing their gender in the same way I was unseen. I perpetrated that bias. I am truly sorry for that.
I dont consider myself trans. Cis does not fit comfortably either. For me, nonbinary means that – actually off the binary. That includes cis and trans, masculine and feminine, as well as good/bad, right/wrong, in/out, victim/perpetrator, love/hate. Unpacking the binary has been an enormous relief on multiple levels. I have a gender euphoria at deeply knowing that I am more than people assume I am from my face. I also still struggle with the words and explanations around what gives me the right to feel like I have a different gender than, for example, my also pierced and tattooed, also radical, also queer femme friends that dont identify as nonbinary.
I have had an image of gender as a 3D nebula with us all bouncing around inside moving through our beautiful multifaceted lives as our original and authentic selves. A few people stick to one pole or another; most of us are all over and in between at any one time. I am grateful for evolving language that imperfectly and accurately outlines a frame for my complex gender despite how you may read my face, my clothes/hair and my genitals. I still feel pretty unsure of the language and philosophy to discuss this evolution though. I have no critical theory or objective framework to reference when it comes to being a nonbinary femme or themme.
I welcome communication from nonbinary femmes out there of any age. Lets have coffee and talk (missmasina@gmail.com).
I add my voice to the growing number of health care professionals and medical societies condemning the newest human rights violation by the Trump administration against our transgender community. The urgency of this issue is paramount! To deny health care rights during a global pandemic is both inhumane and absurd. Our trans patients and colleagues are already vulnerable due to the health disparities inherent in our system and biases from healthcare practitioners. Not only are out trans patients affected but all patients who fall under any part of our QUEER community in the past, present or future are at risk, making it even more difficult to be open and honest wit our health care providers.
Gender based and transphobic violence includes racism, murder and hate crime. It disproportionately affects black trans lives, especially black trans women. In the midst of the Black Lives Matter uprising and Covid19 the reversal of transgender health protections puts an immediate threat to black trans patients, and all trans BIPOC patients who identify as gender neutral or non-binary.
This recent action should be met with a call to arms from all medical professionals, including attending physicians, resident, medical students, nurses, APPs and staff. We must to do our best to provide trauma-based compassionate medicine and NEVER deny care for transgender patients nor any LGBTQ patients. The personal views of providers in any setting (outpatient, clinic, hospital or otherwise) must not be allowed to interfere with the right to health care. The recent COVID pop-up hospital in a Brooklyn park that denied transgender and LGBT care is an atrocious example of what the Trump administration is suggesting here.
There is a dearth of education for healthcare professionals from the earliest academic levels. Health disparities, intersectional oppression, and implicit biases of language, systems and structures have to be called out and addressed to stop this cycle of ignorance. Silence is clearly violence, and we cannot in good faith stay silent and allow conservative politicians to sacrifice health protection in the names of transphobia and racism – not now or ever again.
Kaiser Kabir OMS4 Lincoln Memorial
University
Masina Wright, DO PGY1 University of
New Mexico Hospital, Internal Medicine
Well, I bled for 16/30 days in April plus 5 in May. This is not my normal. This is pandemic menses. I don’t remember the relationships between cortisol, ovarian function and the reproductive cycle and frankly I haven’t had the energy to look it up again. I am also 46, so my ovarian reserves are low and having anovulatory/ short cycles could be the new normal until I get fully into bioidentical hormone replacement land. Still: Why such extended Abnormal Uterine Bleeding (AUB) ? And why this extended pain, expense and moodiness when I am already working long hours, alternating day and night shifts, and having to accept the global panic of COVID?
I have not changed much of my regular hormone regime. I have been taking bioidentical progesterone the second half of my cycle for the past 10ish years. Ovaries start decreasing progesterone production around 35yo often causing worsening PMS, cramps, and shorter lighter cycles. Taking progesterone lengthens my cycle from 21 to 26ish days and really helps with cyclic breast pain, bloating, cravings, PMDD and cramps. I had been on vacation when all this started and had not been taking it consistently 🙁
I also take testosterone as a subQ injection intermittently. It is prescribed as a weekly shot, but I tend to take it only every 2-3 weeks, mostly because I forget. Sometimes I forget to take it for months at a time. Cis female ovaries and adrenals produce small amounts of testosterone throughout the lifetime, and testosterone is the dominant cisfemale hormone of menopause! Endogenous production tends to decrease around age 40 as an average.
When I was working at Age Management Center, I tested dozens of women’s testosterone levels between ages 25-75 and it was extremely common to have very low levels: more common than normal levels! Optimization of this all-gender hormone brings a sense of vitality, physical and mental strength, increased muscle mass, heightened endurance, and improved orgasm strength (or orgasms, maybe for the first time!) It helps me have the energy to get to the gym and enjoy workouts. I also had an improvement in libido and sexual satisfaction. I have been taking this rx more frequently these days as internal medicine is *exhausting* so low T is not at the root of my hormonal shifts.
That leaves estrogen as the possible culprit, and this could certainly be the case.There are 3 different estrogens in the body that can be measured. Estradiol is the major circulating hormone that has all the beneficial effects – elasticizing bone, brain, blood vessels, and skin. Estrone is a metabolite of both testosterone and estradiol through aromatization and is theorized to have more inflammatory and proliferative effects. The ideal Estradiol: Estrone ratio is 2:1in the body. Estriol is the weakest estrogen and is localized to the uterus and vagina. This enhances vaginal lubrication and tissue health. It is also what is typically used for vaginal replacement in menopause or transmasculine health because it has less systemic effects. I am due to go get my hormone levels tested to see of I have had a big shift in estrogen levels. Lab work is ideal when done between days 19-21 of a cycle to catch all 3 hormone levels. I have not had any side effects of low estrogen yet, but as a 46yo, the decrease is coming.
I will likely transition to bioidentical hormone replacement when my ovaries retire fully. Humans used to go into menopause around 50-55 then die around 65. I do not think we were made to live an extra 40-50 years (90 yo) without any gonadal hormones. And as someone who will be in high productivity for many years head working in medicine, I will need these juicy, foundational, resilient, life giving hormones! Plus, I love the feeling of being strong physically, mentally, sexually and emotionally!
What about Breast Cancer you ask? Well, fortunately I do not have the gene that puts me at higher risk. I also eat lots of foods full of plant nutrients, antioxidants, fibers, and phytochemicals and good quality meats and fats. I exercise occasionally, especially out in nature where I can fill my lungs with fresh oxygen. I have a lot of stress in my life, but I do my best to counteract that with affection, loving kindness towards myself, sleep, mindfullness meditation, therapy, strong friendships and sunshine/water/flowers. Estradiol does increase proliferation of breast tissue; bioidentical progesterone counteracts that maintaining a balance of growth and suppression. Testosterone itself is also apoptotic meaning it is anti-cancer/ pro cellular health in nature. For me, in this body, having a well of hormones to draw from as I continue to function in the world is a source of inner vitality that I can give myself, even when my ovaries stop being able to produce it themselves. And, I will probably stop full bHRT after around 15 years, which is what evidence has shown is the time when long term hormone replacement therapy in ciswomen stops being as effective and starts to drift towards harmful. I may even just continue testosterone in those years which has less negative evidence as well as less links to breast pathology.
I have effectively convinced myself this was probably an estradiol dip in ovarian production resulting in a very short cycle partially due to low progesterone followed by an ovulatory but still low estrogen short cycle. Fingers crossed that this is not my new normal. I have also re-upped my commitment to taking my daily thyroid medication as well as adrenal herb supports, because the hormone systems all work in tandem and when one part is dysfunctional, others need to work extra hard. But the adrenal and thyroid systems are a whole other conversation for another day. And maybe I will read up more on the links between stress and hormones between now and then.
Meanwhile, This Gal needs to get ready for her night shift in the COVID ICU. Stress. Yup. Exhausting emotionally and physically. Yup. My ovaries can probably read the cortisol and adrenaline levels in my blood and there may be another month of AUB ahead as my body instinctively tries to preserve its resources for essential functioning only in these pandemic times. At least I know what to do for it! I also did book an appointment with a new gynecologist to have an expert on board in case I need something like imaging or a more extensive workup. A Doctor cant always heal herself!
I went to my local Co-op today, which is one of the only places that doesnt feel totally overwhelming to shop, and every single person had a mask on. This is the new norma I spent the week pretty anxious about the contagion and infectious side of COVID19. I had two of my patients get ruled out for the virus mid-treatment this week AND the contagion aspect seemed really important for those around me I come in contact with, not only myself. What do I need to do to not be a vector of spread? We now only wear scrubs to the hospital not work clothes, and I take my shoes off at my door. Are you freaked out about the contagious side of it? This is a real phobia for some people, and it at the root of many OCD compulsions. I feel for all the germ-phobes out there! My only advice is therapy therapy therapy. There are also one or two antidepressants that help with OCD if you are really noticing an uptick in this in your every day. Ask your PCP if they can help. If you dont have one, this is a great time to get one! Many health providers are accepting new patients, and their clinics or your local community center can help you get the health coverage you need.
Medicine really needs to start valuing mental health as equal to primary and specialty medical care in insurance reimbursements and coverage. SO much suffering comes from the mind. And teeth! Dental coverage too! I promised a blog on botanical medicine and viral illness. I am not up to date on the most current treatments and theories in the natural medicine world anymore. The Naturopathic News and Review publication is a great resource for cutting edge evidence from practicing ND’s.
Most of my botanical training is american traditional eclectic western botanicals, and the knowledge dates back to folk traditions, native medicine, midwifery, and turn of the century medicine. In this vein, there is a wealth of knowledge about foundational immune support and antivirals vs antibacterials and antifungals. If you are interested in this kind of care, most ND’s and herbalists are doing telephone and online appointments and shipping our medicine. Look under your Naturopathic Medicine State Association and see who is available in your area for personalized medicine.
Chinese botanical medicine also has a fantastic apothecary of immune supporting botanicals as well as support for basically every system. Their pharmacopeia is rich and complex with over 5000 herbs with specific indications and formulas. Many TCM Doctors and Acupuncturists are also herbalists and sell custom blended teas as part of their practice. Consider reaching out to someone locally for this as well with a phone or video appointment.
Herbal Medicine for COVID19 falls into prevention by strengthening and prevention by antimicrobial actions. Prevention by strengthening herbs are used when you are not sick. They tonify and strengthen the body, increasing reserves that can be called on if illness occurs. The following is a list of such herbs:
nettles
astragalus
alfalfa
borage
siberian and american ginsengs
ashwahaganda
cordyceps and other nourishing mushroooms (use sparingly)
Nettle Cake with Pine Buttercream
Nettles are best made as a herbal tea and drank clear and often. They can also be eaten in soups, cakes, and stir fried although this is easier in some parts of the country than others.
Astragalus is a sweet root and is best as a broth, or a tablet taken 3 tablets in morning and night. This is a key ingredient in “change of season soup” from the TCM formulary for immune strengthening as well. Borage, Siberian and American ginsengs and ashwahaganda are adrenal tonics that boost immunity by decreasing inflammation and increasing resilience. I like borage tincture 1 tsp daily, ginsengs as tinctures or pills (they don’t taste great), and ashwganda as a standardized tablet or capsule. Ashwaganda means something close to “horse piss” Ive been told, and it is named after the strength and passion of a horse as this is what it embues. These should be discontinued at the first sign of a sniffle or other illness. Then switch to active antimicrobial prevention. Taking these while sick can sometimes strengthen the pathogen rather than the host.
Antimicrobials: These are divided by their functionality.
Use these herbs as a prevention; it is best to preserve the antibacterials for signs of actual infection. Like Rx antibiotics nature’s antibacterials have strong actions and their use needs to be preserved for proper indication
A selection of commonly used antivirals includes:
alium cepa (onion)
allium sativa (garlic)
echinacea – only in the first 24 hours of infection
euphrasia (eyebright) – for viral conjunctavitis and eye symptoms
cats claw
A selection of my fave antibacterials include:
goldenseal – for inflamed mucus membranes and purulent discharges
berberis – for anything that looks or feels “infected” including GI issues
echinacea – one of the only botanicals proven against strep species. Use a glycerite form of the tincture and squirt it directly onto an inflamed throat. The glycerite is sweet and is safe for children and elders.
cats claw – used for Lyme infection
onion and garlic, oregano and thyme – in cooking! use liberally!
Antifungals are also important for chronic immune system depletion often manifested as thick brittle toenails or fingernails, frequent yeast infections, sinusitis and chronic belly issues. They are less relevent for this pandemic other than to sustain and support long term immune and lung health. My go-to antifungals include:
monolauren (from coconut oil) 300mg 2 times/ day
pau d’arco tincture or tea – 2 tsp or cups per day
tea tree oil – topical
caprylic acid – at least 2 caps daily
garlic
* a note on essential oils
I personally took a bottle of astragalus tablets 2 2twice-ish daily and now I am switching to Monolauren daily for 3 months with vitamin C and cats claw tincture daily for at least the next 3-4 weeks for intensive antiviral support. I am also taking ashwaganda as an energy tonic to support my stress levels during this unusual time to be working in medicine, and a probiotic. For my personalized medicine I have an herbal thyroid support formula alongside my Armor thyroid medication as I have Hashimotos thyroiditis. Finally, I drink homemade nettle tea or lavender/ chamomile tea and am doing the best I can to get cooked or fresh greens most days.
My training in essential oils is only for primarily olfactory/ inhaled, diffused in water or skin products. I was not trained in “by mouth” use of essential oils such as promoted by DoTerra or other EO companies so I cannot recommend tfor or against these by mouth. I do like topical and diffused use of these medicinal substances and find myself drawn to tee trea, eucalyptus and lavender, cypress, pine as my primary antimicrobial nature scents for baths, lotions, soaps and diffusion. Many flower essential oils have beneficial effects on the mind/ mental health as CN1 is a cranial nerve. There is a long tradition of use for cosmetic use as well.
Best of luck out there friendly readers. How we as humans conduct ourselves in these pandemic times can illustrate where we need to work on ourselves and where we shine bright. This is an excellent time for insight, awareness and evolution. Its also a perfect time for devolution and hopelessness. Reach out and find the resources you need or ask a friend to listen awhile: many providers are providing sliding scale or free servicesand telemedicine is blooming. The world is small with the internet. Kindness can be found in bugs on a sidewalk or a smiling eyes from 6 feet. If nothing else is true, it is that we are in this together.