This post was originally written for Apothecary By Design in December 2013 http://www.apothecarybydesign.com/blog/
Stop Wasting Money on Vitamin and Mineral Supplements! 5 medical doctors cried out in an editorial piece first released in the Annals of Internal Medicine, and then circulated through all major newspapers and social media outlets early this week. The articles released in the New York Times, Wall Street Journal, LA Times, and countless other newspapers pointed out that multivitamins have failed to show benefit in several large scale studies; however, the evidence reviewed was not as clear as we were led to believe. As with every evidence based study, it is important to look at the information behind the research, the studies cited, and the actual information the studies gathered.
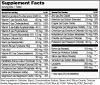
The quality of multivitamins IS a true concern for consumers. The studies supporting multivitamins have been mixed, and we acknowledge this. If you are going to take a multivitamin it is not an effective use of money to buy a low quality product (like the one illustrated below) that is not well absorbed and/or is coated in toxic chemicals and fillers. A very good diet may reduce or eliminate the need for a daily dose of essential nutrients. Some multivitamins may be a waste of money, not because studies illustrate a lack of benefit, but because of the abysmal quality of the product itself. Choosing an appropriate multivitamin is another question – one that Apothecary by Design’s wellness specialists welcome.
The following studies were used to support the evidence that multivitamins are not worth taking:
 1. Multivitamins and cognitive decline in men 65 or older
1. Multivitamins and cognitive decline in men 65 or older
For example, in the first study on cognition, the multivitamin assessed was a well-known common multivitamin that provides low level nutrients in the cheapest, least bioavailable forms. These poor quality minerals generally include oxides and sulphates. For example, magnesium sulfate is epsom salt, like you would use in a bath. Magnesium citrate is a better quality, more absorbable mineral. (See label) Check out the “other ingredients” as well – 3 artificial colors including the noxious FD&C Red #40.
Regardless of the supplement quality, cognition issues are not primarily related to vitamin/ mineral deficiencies, but are a long term response to heavy metal toxicity, poor cerebral perfusion (not enough blood to the brain), omega 3 deficiency, hormone deficiency, environmental contamination, stress and elevated cortisol levels, head trauma, prescription medication side effects and many more individual variants.
For example, how many of the physicians studied were also taking statin drugs? These ubiquitous prescription medications are known to have memory impairment, loss of memory and amnesia as potential side effects.
When presenting strong statements like multivitamins are a waste of money, it is responsible to use evidence that considers a straighter line between cause and effect.
2. Multivitamins failed to reduce cardiovascular events in men and women with previous myocardial infarction
The second study cited as proof that multivitamins are a waste of money was a 2012 study evaluating the effects of chelation therapy on men and women over 65 with history of a heart attack.
This study had significant setbacks. Chief among them were the high drop-out rates due to the strenuous protocol of 30 weekly chemical chelation infusions followed by 10 maintenance infusions two to eight weeks apart.
It is difficult to assess the effect of a multivitamin on long term health with such invasive chemical and vitamin therapies being administered at the same time, and it certainly clouds what is presented as a black and white result.
Antioxidants, nutritional counseling and botanical therapies are also first line treatments in the Integrative health world to repair myocardial function. Once again, the true nature of the study being cited is obscured by the dramatic headlines.
2. Multivitamins did not prevent the development of chronic disease or death.
If only a simple, cheap, low dose, poor quality multivitamins could save the world from chronic disease….
Quality matters in the food we eat, the medications we take and the supplements we buy. Chronic disease is a complex, multifactorial health concern whose cure cannot be reduced to oversimplified statements like these.
Finally – the original article states “….beta carotene, vitamin E and possible high dose vitamin A supplements increase mortality.” What they leave out, is that high dose beta-carotene increases risk of … lung cancer in smokers (only.) And alpha-tocopherol vitamin E increases the risk of heart disease …but full spectrum vitamin E with both tocopherols and tocotrienols reduce the risk. Limiting the information sensationalizes the story, obscures the evidence and limits its relevance.
The great thing about this editorial is that it exposes the poor quality multivitamins out there for what they can be: a sense of false security. No one can eat fast food regularly, take a poor quality low dose multivitamin, not practice any preventative measures, and not develop chronic disease eventually. That much IS true.
A multivitamin needs to be able to be absorbed, with high quality minerals and therapeutic dosages of vitamins at the very least to offer prevention and protection. These remain a worthwhile investment for people wanting to maximize their nutritional value. Furthermore, high quality children’s multivitamins remain a good nutritional adjunct for picky eaters and kids with behavioral or health issues. Multivitamins are not a substitute for a healthy lifestyle with good quality food choices, exercise, and stress reduction.
http://www.mayoclinic.org/medicalprofs/trial-to-assess-chelation-therapy-cvuv10n4.html
http://www.ncbi.nlm.nih.gov/pubmed/10359235
http://www.medscape.org/viewarticle/501471
http://www.nleducation.co.uk/resources/reviews/the-next-generation-vitamin-e-how-tocotrienols-benefit-the-heart-brain-and-liver/
Enough Is Enough: Stop Wasting Money on Vitamin and Mineral Supplements. Annals of Internal Medicine. Eliseo Guallar, MD, DrPH; Saverio Stranges, MD, PhD; Cynthia Mulrow, MD, MSc, Senior Deputy Editor; Lawrence J. Appel, MD, MPH; and Edgar R. Miller III, MD, Phd p. 850